In the world of Preimplantation Genetic Testing (PGT), we begin with an embryo biopsy. The quality of the biopsy is not always the same, in order to extract the sufficient amount of DNA for testing, the biopsy must be performed precisely.
With the current tendency for blastocyst transfer (day 5-6 of human embryo development), there is a prevailing interest in the blastocyst biopsy, performed for PGT, which has already resulted in numerous successful IVF cycles, with normal clinical pregnancies and the births of healthy children.
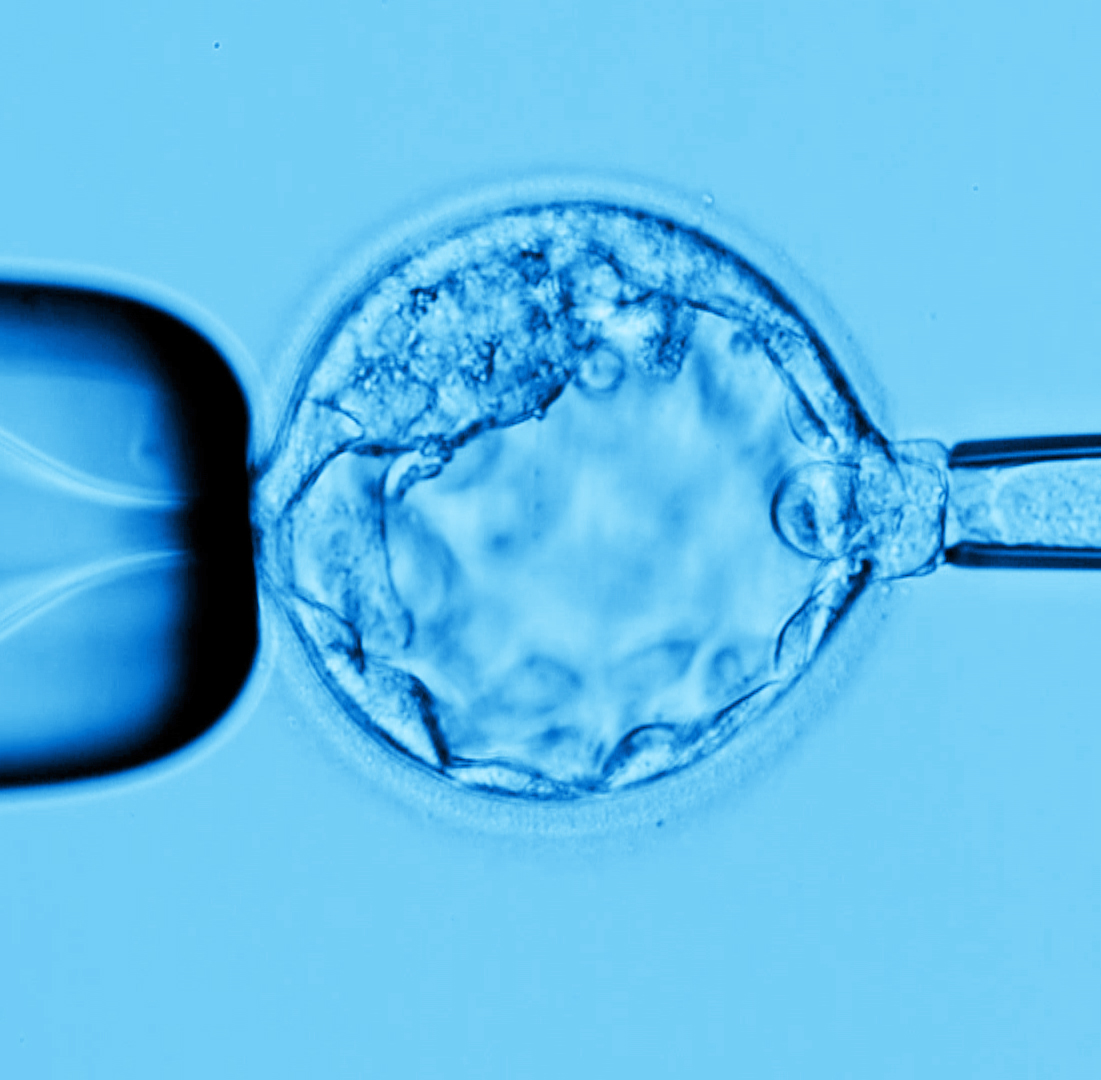
A blastocyst biopsy is performed on an expanded blastocyst with the use of a laser; several trophectoderm (5 to 7) cells are removed by gentle aspiration using a biopsy pipette with an internal diameter of 25 µm. On average, a blastocyst contains more than 100 cells. The trophectoderm, the area from which the cells are removed, ultimately becomes the placenta. Therefore, removal of a few cells from the trophectoderm is very unlikely to have a detrimental effect on the blastocyst’s development, particularly on the development of the fetus originating from the inner cell mass.
The Blastocyst biopsy became a method of choice for most of IVF laboratories, including RGI, and currently has a growing potential in the improvement of freezing techniques, particularly embryo vitrification. It became especially effective with the introduction of Next Generation Sequencing (NGS) technology for aneuploidy testing of all 24 chromosome know as PGT-A, which provides significantly more accurate and reliable results when performed on a blastocyst biopsy. Having many cells to test prevents hybridization and amplification failures. It also prevents misdiagnosis in mosaic embryos which may have both normal and abnormal cells, thereby increasing the reliability and accuracy of the diagnosis.
You can see Day 4 and Day 5 biopsies performed in our laboratory on the RGI YouTube channel:
By: Yuri Ilkevich, Director of Micromanipulation, RGI
In case of maternally derived genetic mutation, polar body biopsy has its prominent advantages in PGT. In addition to the blastocyst biopsy, is polar body biopsy still be adopted in RGI?
We review polar body testing requests on a case by case basis.